Mixed-signal PCB
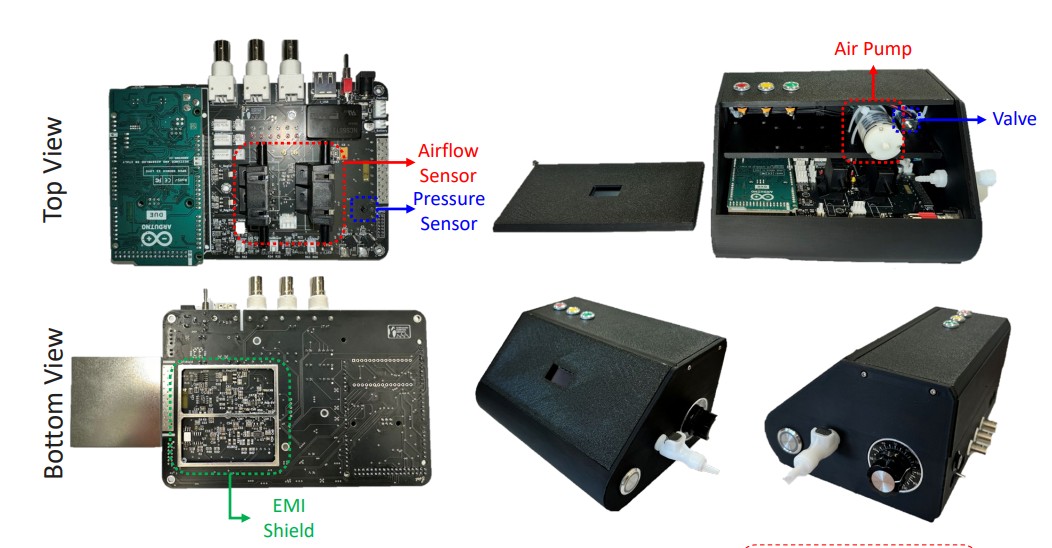
Custom 4-layer board with pump/valve drivers, instrumentation amp for cuff pressure, ECG AFE, MCU, and isolated USB. Designed end-to-end — schematics, layout, BoM, bring-up.
Flagship project · $2.7M NIH-funded · multi-site clinical study
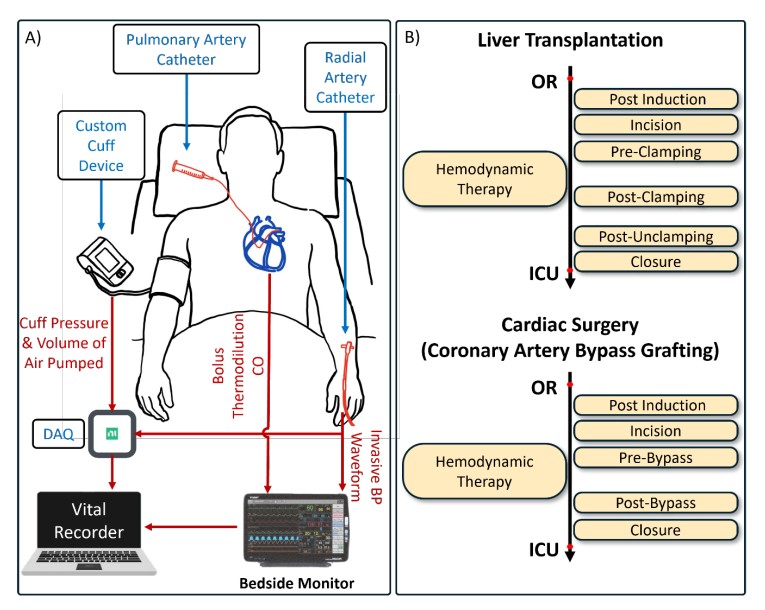
A regular arm cuff — rebuilt from the analog front-end up — that estimates cardiac output, blood pressure, ECG, and respiration in one cycle. Validated against catheter-based gold standards in 34 surgical patients.
Hospital-grade hemodynamic monitoring — the kind that decides whether a patient on bypass needs a fluid bolus or a vasopressor — runs on catheters threaded through the chest. Catheters are accurate. They’re also invasive, expensive, and unavailable outside the OR or ICU.
Smart Cuff asks a different question: how much of that information lives in the brachial artery, where a $30 cuff already sits? My answer, after three years of hardware, firmware, signal pipelines, and clinical data: more than the field assumed.
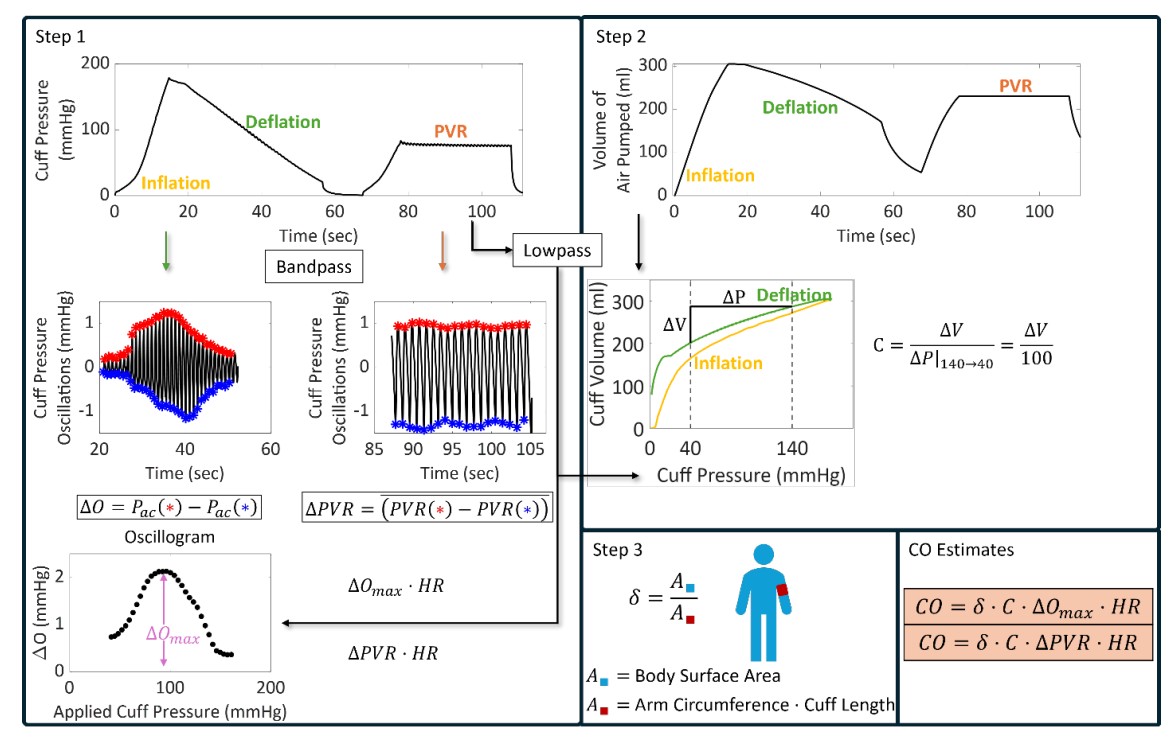
One automatic cuff inflation gives us four physiological windows — the pneumatic pressure trace, an ECG lead, the cuff-coupled respiration signal, and the oscillometric envelope itself. From those four, with the right physics-informed model, the cuff estimates cardiac output, BP, HRV, and respiratory rate — in one shot, no catheter.
That correlation isn’t world-changing on its own — but matching what an invasive pulse-contour catheter delivers, without putting one inside the patient, is. The point isn’t replacing the catheter in the OR. It’s extending hospital-grade monitoring to the wards, the post-op floor, and eventually the home.
Closed-loop PID drives the pump up past 180 mmHg, pinching the brachial artery shut. The pressure trace becomes a clean carrier we can subtract out later.
Calibrated valve releases air at a controlled rate (~3 mmHg/s). The artery reopens once per heartbeat in the band where transmural pressure crosses zero, leaving a tiny oscillometric ripple on top of the slow ramp.
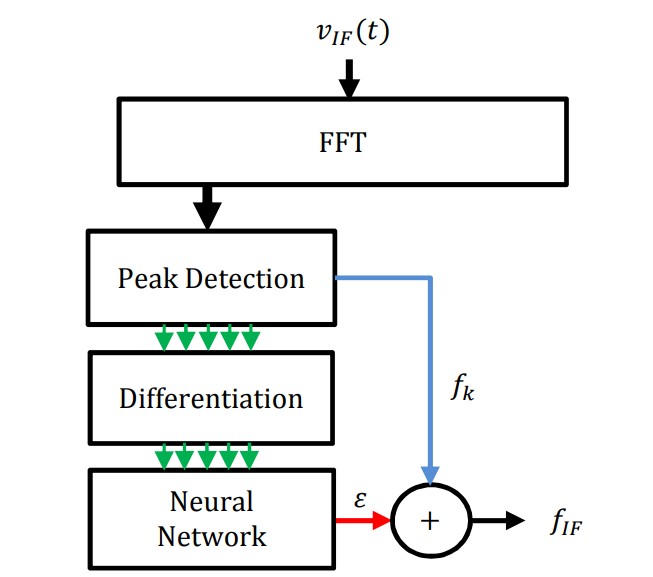
Bandpass + harmonic-SNR gating pull the oscillometric envelope out of the cuff signal. ECG comes in cleanly on its own front-end; respiration shows up as a slow modulation on the cuff baseline.
Pulse pressure, envelope shape, R-to-pulse delay, and beat-to-beat amplitude variance carry independent information about stroke volume, vascular tone, and respiratory loading.
A small neural network maps physics-derived features to cardiac-output estimates. Trained against PAC thermodilution, regularized hard, kept honest by held-out patients.
Quality gates reject windows where the harmonic SNR is too low, motion artifact too high, or arrhythmia confuses the envelope. A bad estimate is worse than no estimate.
Custom 4-layer board with pump/valve drivers, instrumentation amp for cuff pressure, ECG AFE, MCU, and isolated USB. Designed end-to-end — schematics, layout, BoM, bring-up.
Two-loop control: outer pressure setpoint, inner valve duty cycle. Anti-windup, slew limiting, and venting interlocks so a wedged valve can’t over-pressurize the cuff.
Each valve gets a piecewise-linear flow-vs-duty curve. Re-cal procedure in the GUI takes ~30 seconds per device and survives months of bench use.
PyQt6 protocol runner: pre-flight checks, safety thresholds, real-time PPG/ECG/pressure plots, event annotation, CSV/EDF export. Two clicks from idle to recording.
Hold below DBP, push beat-to-beat tracking into the wards. Pressure-dependent amplification with on-line recalibration — the safety story is the work.
A single number per measurement, derived from harmonic SNR, motion, and arrhythmia detection. Bad readings get rejected before a clinician ever sees them.
Same pipeline, smaller pump, lower duty cycle. Strip the OR-grade ECG, keep the cuff. Unattended morning and evening readings for heart-failure and post-op patients.
Happy to walk through the pipeline, the clinical study design, or the hardware. Email is fastest.